
Despite extensive training in stress management and resilience strategies, healthcare professionals consistently report difficulty translating knowledge into real-time behaviour. This gap is not a failure of motivation or competence—it reflects fundamental principles of human behaviour under conditions of cognitive load, emotional intensity, and time pressure.
This chapter introduces an evidence-based framework for understanding why resilience skills often fail to transfer into practice and how they can be systematically embedded into daily clinical routines. Drawing from behavioural science, cognitive psychology, and implementation research, participants will learn how to convert abstract knowledge into automatic, sustainable habits.
A central insight from behavioural science is that knowledge does not reliably predict behaviour, particularly in high-stress environments such as healthcare.
Under conditions of fatigue, time pressure, and emotional strain, the brain prioritises efficiency over deliberation. According to Dual-process theory, human behaviour is governed by two systems: (Kahneman, 2011)
· System 1 (automatic): fast, habitual, low-effort
· System 2 (deliberate): slow, effortful, reflective
In clinical environments, System 1 dominates due to cognitive load and decision fatigue (Kahneman, 2011). As a result, healthcare professionals default to existing habits rather than newly learned strategies, regardless of intention or awareness.
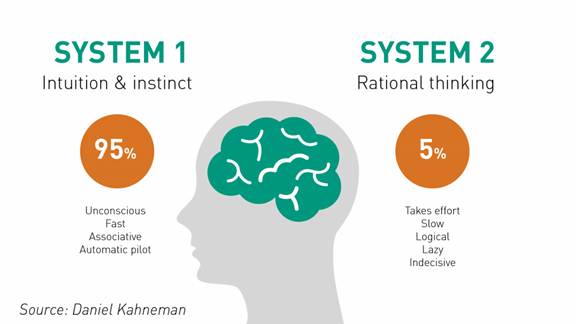
Source: https://www.rogerleishman.com/2017/12/thing1.html
Dual Process Theory in psychology explains how human thinking and decision-making rely on two interacting cognitive systems: one fast and automatic, the other slow and deliberate. It provides a foundation for understanding intuitive versus analytical reasoning, cognitive biases, and the limits of rationality in everyday judgment and behaviour.
VIDEO: Dual Processing Explained
Behavioural research demonstrates that sustainable behaviour change occurs through repeated activation of a habit loop:
· Cue (Trigger): a specific, consistent context or signal
· Action (Routine): the behaviour performed
· Reward: a reinforcing outcome that strengthens the loop
This framework, extensively studied by Wendy Wood and others, shows that context-driven repetition—not motivation—is the primary driver of long-term behaviour change (Wood, 2021).
Even when healthcare professionals are trained and motivated, multiple barriers interfere with real-world application:
1. Time pressure and cognitive overload
Healthcare environments demand rapid decision-making under continuous interruption. Cognitive resources are limited, and under overload, non-essential behaviours—including resilience practices—are deprioritised (Kalisch & Aebersold, 2010).
2. Emotional resistance
In high-stress moments, individuals may experience internal resistance:
“I don’t feel like doing this right now.”
Emotion regulation research (Gross, 2015) shows that stress reduces the likelihood of initiating effortful regulatory behaviours.
3. Absence of triggers or reminders
Without clearly defined cues, even well-learned techniques are not activated at the right moment. Behaviour remains intention-based rather than context-driven.
4. Perfectionism and All-or-Nothing Thinking
Healthcare culture often reinforces high performance standards. This leads to cognitive patterns such as:
· “If I can’t do it properly, there’s no point doing it.”
Research on self-compassion and clinical performance (Germer & Neff, 2013) indicates that this mindset significantly enhances behavioural consistency and persistence by reducing self-critical responses after setbacks.
Effective resilience integration requires designing behaviours that align with how the brain naturally operates under pressure.
1. Tiny Habits Approach
Developed by BJ Fogg, this approach emphasises starting with extremely small, achievable actions.
Example:
Instead of “practice mindfulness daily,” → “take one slow breath after each patient interaction.”
Smaller behaviours reduce activation energy and increase repetition likelihood, leading to faster habit formation (Fogg, 2020).
2. Environmental cues (Context anchoring)
Habits become automatic when linked to stable, recurring events in the environment.
Healthcare-specific examples:
· After hand hygiene → take one breath
· Before entering a patient room → brief pause
· After documentation → cognitive reset
If behaviour is not tied to context, it will not be reliably executed.
3. Pre-Commitment (Implementation intentions)
Structured “if–then” planning significantly increases follow-through:
· “If X happens, then I will do Y.”
Example:
“If I feel overwhelmed during a shift, then I will pause and take one breath.”
Meta-analytic evidence (Gollwitzer & Sheeran, 2006) shows that implementation intentions can double the likelihood of behaviour execution.
4. Social and accountability mechanisms
Behaviour change is reinforced through social context:
· Peer check-ins
· Team-based micro-practices
· Shared commitments
In healthcare teams, social norms strongly influence behaviour adoption and sustainability.
This exercise translates theory into immediate practice.
Step 1: Select one resilience behaviour
Choose a behaviour that is:
· Simple
· Quick (<30 seconds)
· Feasible within your workflow
Examples:
· Brief pause
· One deep breath
· Cognitive reframing
Step 2: Define your habit loop
Trigger (Cue):
“When ______ happens…”
(e.g., “When I finish writing a patient note…”)
Action (Behaviour):
“I will ______”
(e.g., “I will take one slow breath.”)
Reward (Meaning/Outcome):
“This helps me ______”
(e.g., “This helps me reset and refocus before the next task.”)
Implementation guidance
· Keep the behaviour minimal
· Attach it to a consistent cue
· Focus on repetition, not intensity
· Expect imperfection—consistency builds automaticity
Sustaining mental resilience in healthcare requires more than isolated techniques—it depends on the ability to continuously adapt behaviour in response to real-world demands. High-performing clinicians do not rely on static strategies; instead, they engage in ongoing cycles of intentional action, feedback, and adjustment.
This chapter introduces the Plan–Do–Reflect–Adjust cycle, a structured self-regulation framework grounded in behavioural science, experiential learning theory, and performance psychology (Taylor et al., 2013). The model enables healthcare professionals to test, evaluate, and refine resilience behaviours in real clinical environments, supporting long-term habit formation and adaptive expertise.
A key principle from behavioural and learning sciences is that effective behaviour change is iterative rather than linear. Individuals do not simply “decide” and sustain new behaviours; instead, they refine them through repeated cycles of action and feedback.
This aligns with models such as Experiential learning and self-regulation frameworks in performance psychology, which emphasise:
· Action in real contexts
· Reflection on outcomes
· Continuous adjustment
In healthcare environments—characterized by unpredictability and cognitive load—this cyclical approach is essential. Initial plans often fail under real conditions, making adaptation, not perfection, the primary driver of success.
Experiential Learning, as defined by David A. Kolb in 1984, is a holistic learning theory describing knowledge creation through the transformation of experience. It views learning as an ongoing cycle where individuals engage in experience, reflect upon it, conceptualize what they have learned, and then actively experiment with new ideas. This framework underpins much of modern constructivist and learner-centered education.
VIDEO: The PDSA cycle 101
Scope of the video is an introduction to the Plan-Do-Reflect-Adjust Cycle.
1. PLAN
Define the intended behaviour clearly and contextually.
· What will I do?
· When and where will I do it?
Specific planning increases execution likelihood by reducing ambiguity and decision fatigue (Gollwitzer & Sheeran, 2006).
2. DO
Execute the behaviour in a real clinical context, not in ideal or controlled conditions.
· Focus on implementation, not perfection
· Accept variability and constraints
Behaviour must be tested under the same conditions in which it is expected to occur.
3. REFLECT
Evaluate the experience immediately or shortly after execution.
· What worked?
· What didn’t work?
· What did I feel or notice?
· What did I learn?
Reflection activates metacognitive processes—thinking about one’s thinking—which enhances learning transfer and behavioural adaptation (Schön, 1983; Mann et al., 2007).
4. ADJUST
Modify the behaviour to increase feasibility and sustainability.
· Make it smaller
· Make it easier
· Make it more realistic
Behavioural flexibility is a stronger predictor of long-term adherence than initial performance quality (Wood, 2021).
Context:
A nurse is working a busy shift with multiple patients, frequent interruptions, and time pressure. While administering medication, another patient calls urgently, and a colleague asks for assistance at the same time. The nurse feels increasing stress and cognitive overload.
PLAN
· “When I feel overwhelmed during multitasking or interruptions, I will pause for one breath before moving to the next task.”
DO
· During the shift, multiple demands occur simultaneously
· The nurse notices rising stress and attempts the pause
· Execution may be partial (e.g., shortened pause, delayed awareness)
REFLECT
· What worked?
The brief pause helped create a moment of mental clarity before switching tasks
· What didn’t work?
The nurse remembered the strategy only after stress had escalated
· What did I feel?
Initial tension and urgency, followed by slight reduction in overwhelm
· What did I learn?
The strategy is helpful but needs an earlier trigger
ADJUST
· Modify the plan to improve feasibility:
“Every time I finish administering medication, I will take one breath before responding to the next demand.”
Apply the cycle to your own clinical context.
Step 1: PLAN
Identify one upcoming situation:
· A meeting
· A difficult patient interaction
· A high-pressure clinical task
Define:
· Situation: “In the next ______…”
· Trigger: “When ______ happens…”
Step 2: DO (Behaviour Definition)
Specify one small, actionable behaviour:
· “I will ______”
(e.g., pause, breathe, reframe, slow down response)
Step 3: REFLECT (Pre-Structured Prompts)
Some reflection prompts to use after the event:
· What did I actually do?
· What worked well?
· What was difficult?
· What did I notice emotionally or physically?
· What would I change next time?
Implementation Guidance
· Focus on realistic execution, not ideal performance
· Expect partial success—this is part of the process
· Use reflection as a learning tool, not self-criticism